The Largest Accessibility Gap in the Modern Workplace
Your office may have wheelchair ramps and braille signage, but it's still inaccessible for a major portion of your workforce.


Ask anyone to picture an accessible, inclusive workplace. They will paint the same image. Wheelchair ramps, accessible restrooms, braille signage, quiet rooms for the neurodiverse, a mental health day policy. It is a reasonable picture. It is also incomplete.
It is missing the one accommodation that likely affects up to half of your workforce but is not on any accessibility checklist - yet. Here are three stories that explain why it absolutely should be.
Three Stories
The first is Angela. She was a happy kid - top of her class, no particular problems. Then, in 6th grade, everything changed. She started to have trouble focusing. She kept sneezing, was plagued by headaches, and her grades collapsed. Her doctors diagnosed her with ADHD and put her on medication. But still, she didn’t get better. Nothing worked. She continued to struggle until, two years later, she moved to a different school building. Every single symptom magically disappeared.
The second is AJ. Four years into running his HVAC business, he started getting panic attacks. Once every six months at first. Then weekly. Then daily. Then ten times a day. Then full-blown seizures. His doctors ran every test they had, trialed dozens of medications, and eventually concluded he needed brain surgery. Yes, you read that correctly - brain surgery. He had given up hope entirely when someone asked him a question no doctor had thought to ask.
The third is my wife, Jess. She had asthma as a child but grew out of it as she got older. Then she visited me while I was living in Beijing. She started feeling terrible. She was constantly coughing and struggled to breathe at times. It got to the point where we started half-jokingly tracking her coughs per minute as a KPI.
You have probably worked out what connects all three of these stories. But they are not the only ones who share this connection.
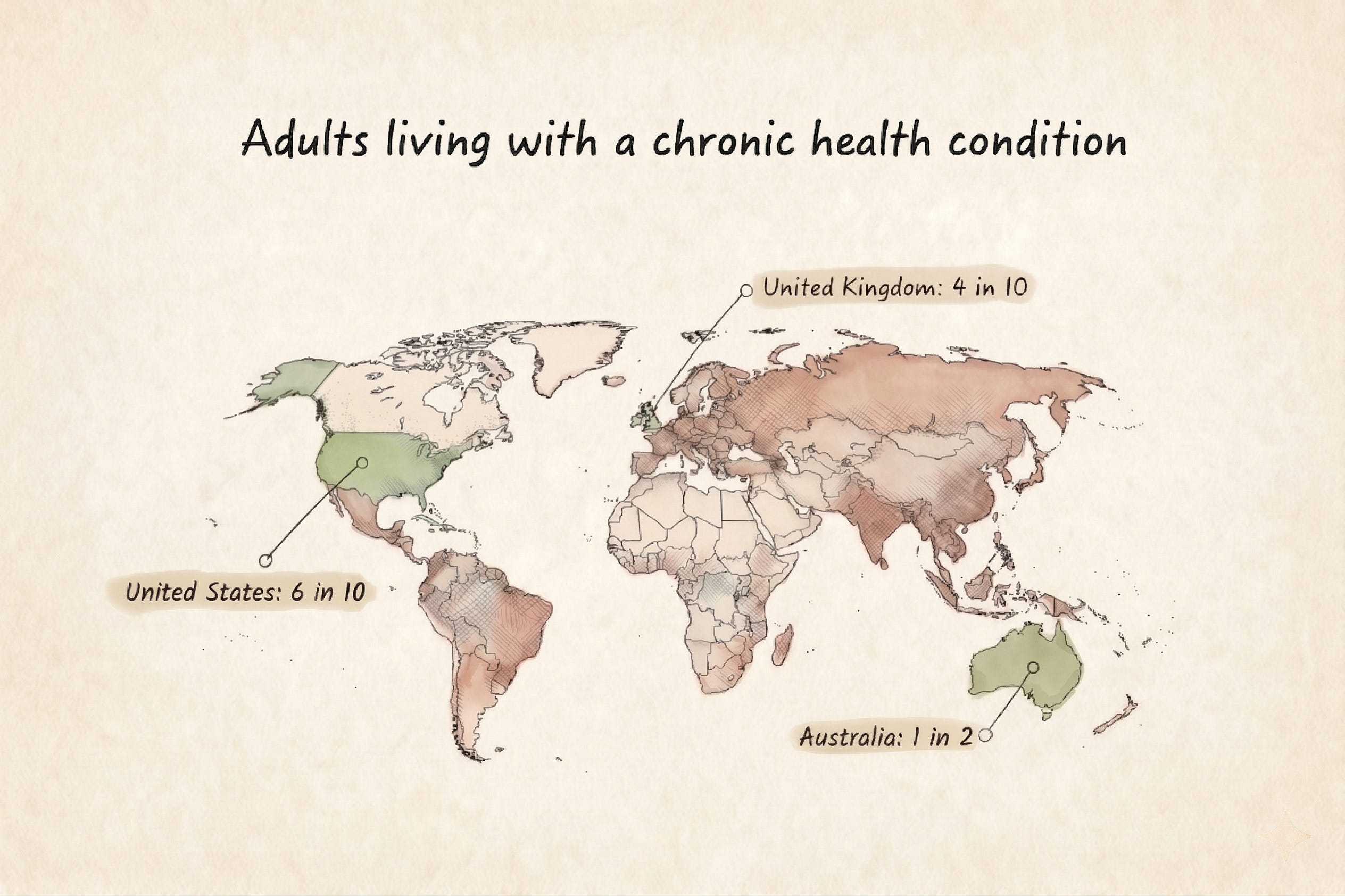
These are not outliers. These are the people in your open-plan office right now - sitting three desks over, managing something you may not know about, breathing the same air as everyone else, hoping it isn’t making them worse.
The Common Variable
Angela, AJ, and Jess are like everyone else on that map. Real people living ordinary lives, whose health, productivity, and quality of life were being systematically destroyed by something none of them could see: the air they were breathing.
In Angela’s case, construction in her school building was generating toxic particulate matter that her doctors never thought to test for. Move buildings, symptoms vanish. For AJ, his occupational exposure to mold in poorly ventilated spaces was the cause of a neurological crisis that very nearly ended in unnecessary brain surgery - until someone asked him, “How’s your air?” For Jess, the severe outdoor air pollution of Beijing - seeping into buildings without adequate filtration - reactivated a respiratory condition she had left behind in childhood.
Three people. Three very different lives. One common variable hiding in plain sight.
The Accessibility Gap
The case for accessibility rests on a simple premise: a physical environment that prevents someone from entering, functioning in, or thriving within a space is discriminatory. We build ramps because a staircase-only building excludes wheelchair users. Braille signage exists because visual-only signs exclude those with vision impairments.
By that same logic, a building with poor indoor air quality excludes an entire population - one that is much larger than the population served by ramps.
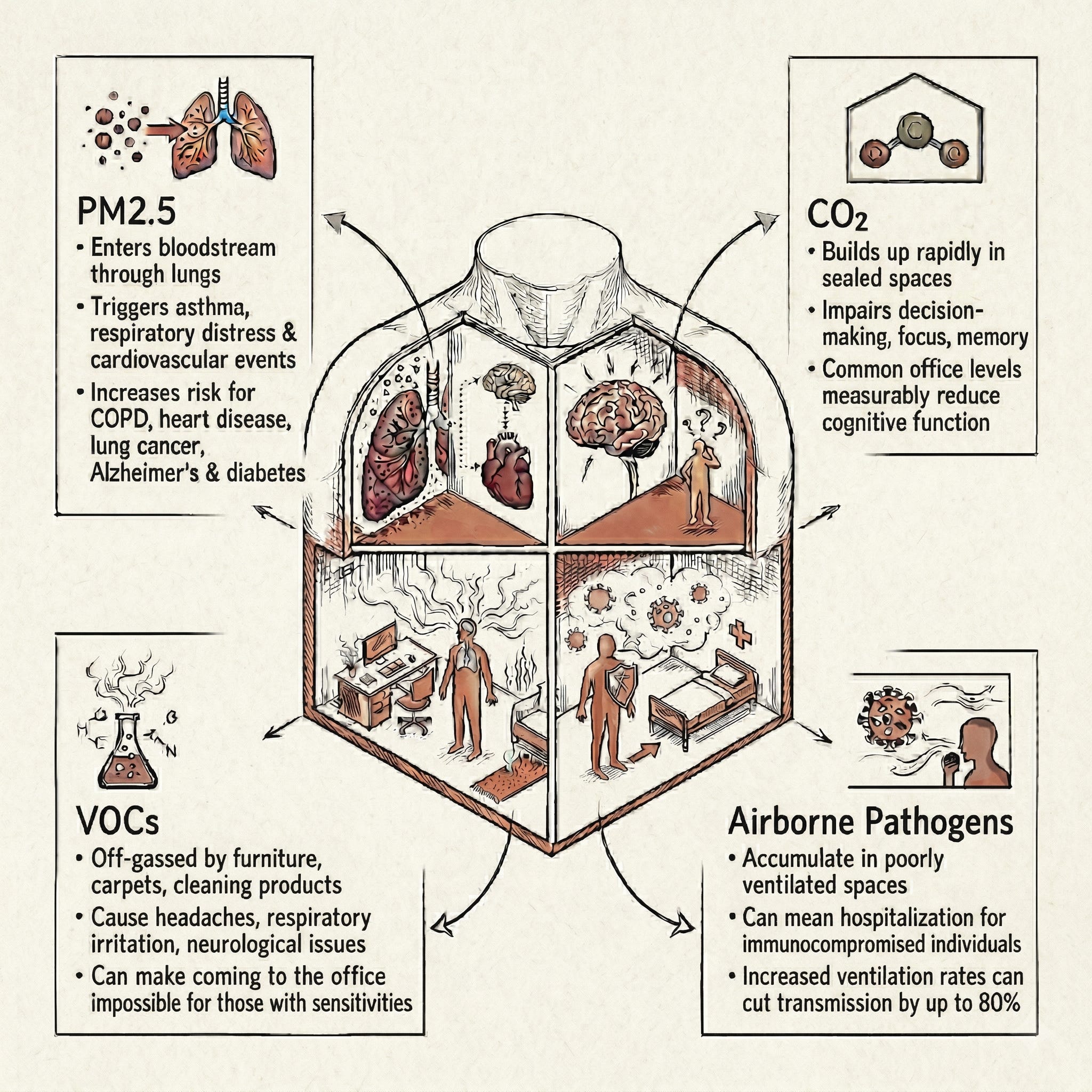
Roughly 9% of the global population has asthma, directly aggravated by particulate matter, VOCs, mold spores, and other toxins.
Between 10% and 30% of people have allergic rhinitis, similarly sensitive to indoor air.
Approximately 7% are immunocompromised at any given time - cancer patients, organ transplant recipients, people on immunosuppressive medications, and those with primary immune deficiencies. For them, a poorly ventilated room is a serious clinical hazard, not a mere inconvenience.
Add COPD, cardiovascular conditions exacerbated by PM2.5 exposure, and neurological conditions sensitive to VOCs and CO2, and the figure balloons.
Despite cumulatively representing up to half the workforce in most countries, this population rarely appears in workplace policies in any meaningful way. At best, they are absorbed into a blanket disability category - one many do not self-identify with. A person managing lupus does not think of themselves as disabled. A cancer survivor returning after treatment does not raise their hand in the accessibility survey. But they are directly and immediately affected by the quality of the air they walk into every morning.
The Most Dangerous Assumption in Real Estate
The natural response from anyone responsible for a building is: “I agree this matters, but our air isn’t that bad.” Ask for proof. They go silent.
The percentage of building managers and workplace leaders with actual data on their indoor air quality is vanishingly small. Most assessments (when they happen at all) are periodic manual inspections. This is the rough equivalent of checking a patient’s blood pressure once a year and concluding they have no cardiovascular risk.
The data from buildings that have actually measured their performance is not reassuring. Take this recent nationwide commercial portfolio audit as an example:
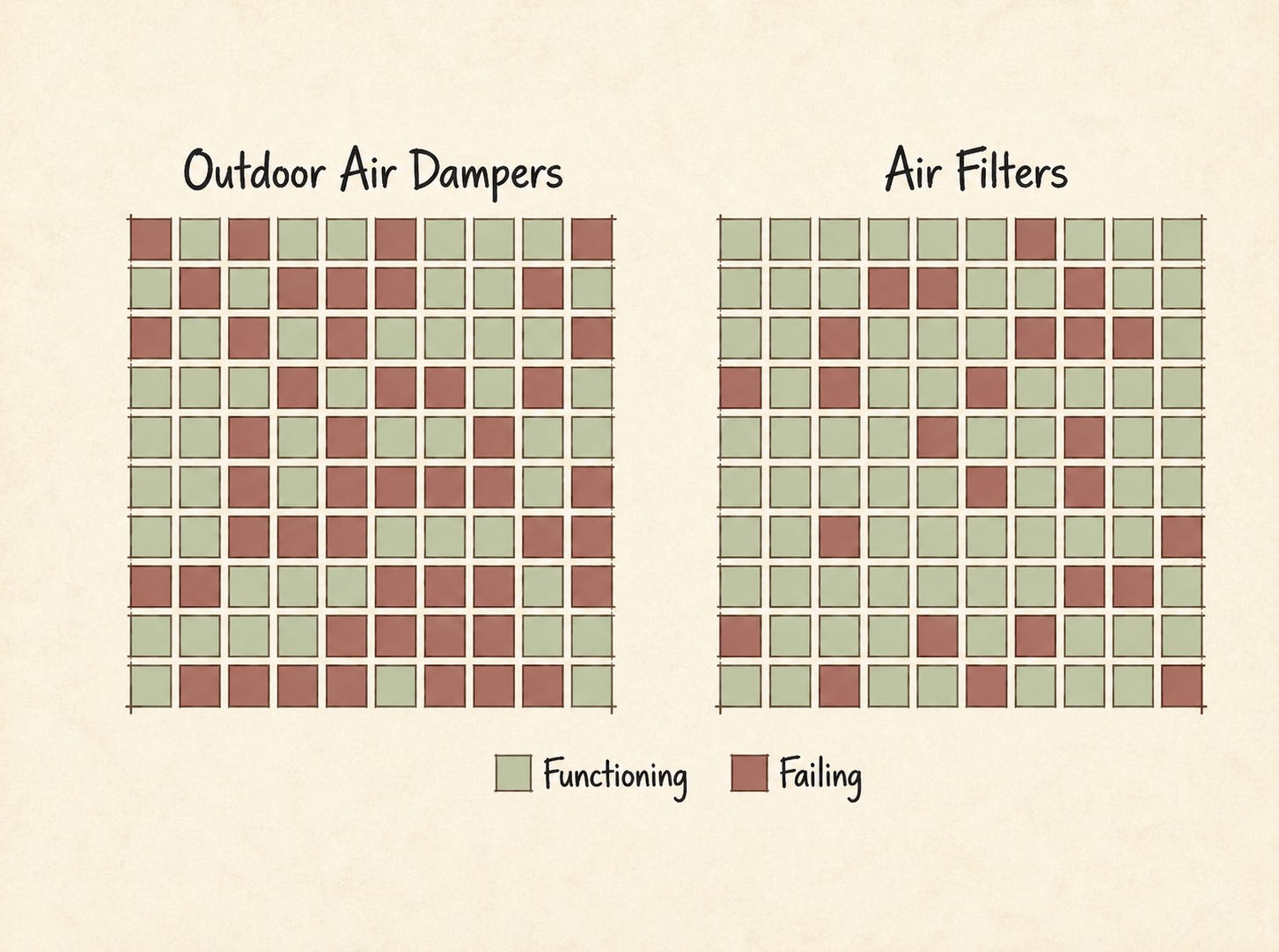
Only 52% of outdoor air dampers and 75% of air filters were in working condition. Many of these buildings failed to bring in sufficient fresh air and filter out particulate matter. Occupants were breathing recycled, polluted air without knowing it.
This is not uncommon. HVAC systems fail silently. Filters clog. Dampers seize. CO2 builds up. The building looks and feels the same whether the systems are functioning or not. There is no broken staircase to photograph. There is just air, the assumption that it is fine, and the slow accumulation of health consequences for the people breathing it every day.
What Good Actually Looks Like
The fix is not complicated. Continuous air quality monitoring gives building managers data instead of assumptions. MERV 13 or higher filtration provides meaningful protection against particulate matter and airborne pathogens. Properly engineered mechanical ventilation ensures shared spaces are not accumulating hours of exhaled CO2.
None of this is experimental. It is widely deployed in high-performance commercial buildings, and within reach of any organization that chooses to prioritize it.
We regulate tap water to a standard that protects the most vulnerable, not the least. We do not accept assurances that the plumbing is “probably fine.” We measure it, certify it, and hold it to a standard. The air in those same buildings deserves the same treatment.
The Decision
The air in most workplaces is excluding countless people, right now. Not by design. By default.
It excludes the person with asthma who spends the afternoon foggy and breathless. The worker with VOC sensitivities who cannot be in the building on cleaning days. The immunocompromised employee who contracts an infection in a poorly ventilated meeting room.
None of this shows up in an accessibility audit or triggers a complaint. It is never fixed because it is invisible - and it stays invisible because nobody measures it.
The ramp did not appear because someone asked nicely. It appeared because someone decided exclusion was unacceptable. Make the same decision. Measure your air, fix what you find, and keep it that way.
Inspired by Plum Stone, founder and CEO of the Safer Air Project. A 20-year veteran of health policy, Plum is the primary driver of the conversation around IAQ as a critical inclusion issue. Through the Safer Air Project, she works to make indoor spaces healthy and accessible for everyone - especially those with chronic conditions.
Absolutely true! Just because we can't see it doesn't mean it doesn't affect us. Recently the change of seasons and no longer needing to run the furnace I switched off the heat not realizing it also turned off the fan which I run all the time to circulate the air in my home. For weeks I was sneezing and dealing with a constant runny nose. I didn't realize the air circulation had been turned off. I have a UVGI light in my return air duct and I was no longer feeling those benefits without the circulation of air. Once I realized the fan wasn't running it all made sense. Turned the fan back on and within hours the sneezing and constant runny nose ended!